The mask/no mask controversy rages throughout the United States. A key factor in the confusion is that multiple public health agencies have flip-flopped on their recommendations. It’s difficult to know who to believe. Even while some are saying, “masks don’t work!” the media and American medical groups bombard us with claims that “the science doesn’t support” the rejection of masks as useful.
The World Health Organization (WHO) has some of the most measured recommendations about masks — and for good reason. Despite the hype, most studies are far more nuanced than what we’re led to believe. I want to take a closer look at one of their own studies, as an example of how studies can be over-simplified to support (or reject) masks…and many other matters in the medical world.
The WHO Mask Analysis
There are several papers that are being used to support the wearing of masks. One is this one from the World Health Organization.
This study is a meta-analysis. What does that mean? It means that the WHO did not directly conduct a study comparing mask wearers to non-mask wearers. Instead, they looked through all the existing studies, found the ones that were relevant to their question, and grouped the data from those studies so they could analyze it as one large group.
One reason this particular study is helpful to look at as an example is that they included a reader-friendly breakdown of the main data points (facts) from the studies that comprised their larger group, so we can see how they’re the same and how they differ.
They looked for studies examining the transmission of COVID-19, SARS, or MERS, which are closely related. The overall findings were that with masks, the transmission rate was 3.1%, versus 17.4% with a mask. This is the part we keep hearing about. But what else do we know about/from this study that might tell us more about when and where these findings are relevant?
Physical Distancing
This study looked at masks, eye coverings, and physical distancing separately. When combining the relevant studies, we’ve seen that masks reduced the rate of transmission from 17.4% to 3.1%. When looking at the relevant studies, this meta-analysis also found that physical distancing reduced the rate of transmission — from 12.8% to 2.6%. This was on average, and increased distances seemed to result in increased reduction.
(The percentage without distancing is different from the percentage without masks because different groupings of studies looked for this information.)
This is the basis of the WHO’s recommendation that masks be worn when physical distancing is not possible.
Setting
The studies that are gathered together for this meta-analysis were conducted in a variety of settings. Many were in healthcare settings, and the researchers separated these for further analysis.
In a healthcare setting, the impact was more pronounced — 7.4% without masks, 3.6% with, versus 20.9% reduced to 15.1% outside healthcare settings. As we’ll see shortly, that may be due to the type of mask worn, rather than, or in addition to, the location.
The studies outside the hospital varied. Most were households and close contacts. One was a dormitory, which is similar to a large household. A couple are described as “community,” which is not completely clear as a designation. One was an airplane. The important takeaway here is that, as a whole, this does not represent the kind of situations (grocery shopping, etc.) where the public is being encouraged or instructed to wear masks.
Type of Mask
Part of the increased benefit of masking in the healthcare setting may be the more frequent use of N95 respirator-style masks. Although the study overall included N95 respirators, disposable surgical masks, and “similar [to surgical masks] reusable 12–16-layer cotton masks,” the authors also identified which were respirators and which were masks.
In the mask group (in healthcare settings), the masks reduced transmission from 28.5% to 16%. N95 respirators reduced transmission from 4.5% to 0.7%.
You may have noticed that in the respirator studies, even the control groups had much lower transmission. This might suggest that facilities that tend to use N95 respirators also tend to take greater care in general with regard to containment of contagion.
Location
Continuing with the theme of variations in degree of hygiene, we might expect to see variations in transmission between certain countries. So what about the United States? Four of the studies were conducted in the United States (all in healthcare settings). In these U.S. studies only, use of a mask or respirator reduced transmission from 3% to 0%.
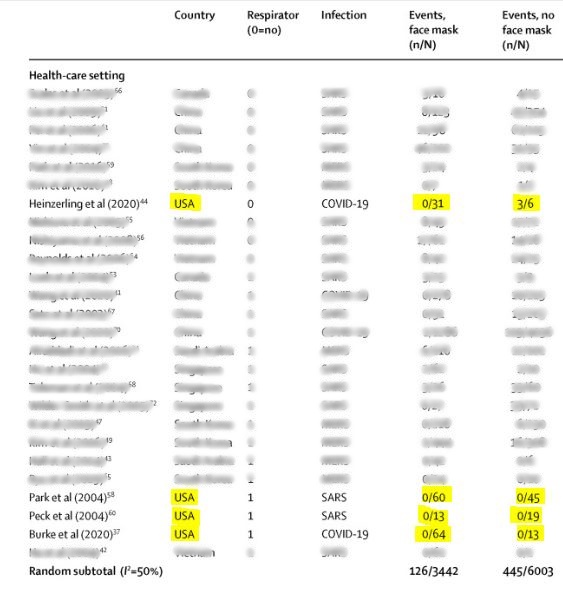
In fact, in three of the studies, there was 0 transmission in both the study group and the control group.
The exception was a study (report) where three healthcare workers contracted COVID-19 after working with a patient without a mask. This was a patient with severe respiratory distress, receiving heavy intervention, such as “nebulizer treatments, bilevel positive airway pressure (BiPAP) ventilation, endotracheal intubation, and bronchoscopy.” In other words, this was a scenario where the most avid non-maskers would consider the use of personal protective equipment (PPE) sound practice!
Summing Up
What I hope you’re seeing is that what is true isn’t necessarily the whole picture. The meta-analysis showed a reduction from 17.4% to 3.1% when a mask or respirator was worn, and this indicates that there is some context in which this type of protection is apparently effective.
But when we break it down, we find there’s little here to indicate anything about wearing a mask in general community contexts, in the United States, where one is not typically within about 3 feet of other people, while apparently healthy.